

This regular update accompanies the post 'The Likely Progress of COVID-19 in the UK'
Analytical Appendix (last full update, 18 May)
The purpose of the Appendix is to present the background data and analysis behind the ‘forecasts’ in the main blog.
There is no substitute for detailed epidemiological modelling of the virus,[1] particularly for examining the impact of interventions on key parameters such as the ‘reproduction number’, and these analyses are clearly important for forecasting the progress of COVID-19 in different countries. These models do, however, depend on many parameters, leaving room for complementary analyses for forecasting purposes. In this note, I report an approach that is transparent and easy to understand. It focuses on deaths in all settings reported by Public Health England (PHE), not just deaths in hospital, and relies on the development of deaths in countries further along in the epidemic (Italy and Spain) to forecast future mortality, as does the epidemiological modelling cited above. It also examines confirmed cases using a similar methodology, and it contains a detailed discussion of ‘excess deaths’ in England and Wales.
UK Deaths
Data on Covid-19 deaths in the UK are produced by Public Health England (PHE). Deaths reported from three sources are linked to the list of people who have had a diagnosis of COVID-19 confirmed by a PHE or NHS laboratory. This is to identify as many people with a confirmed case who have died as possible (https://coronavirus.data.gov.uk/about#process-from-29-april-2020.) These data became available on 29 April, and they replaced the previous series of confirmed cases dying in hospital reported by the NHS. This new series of deaths includes all deaths previously reported by NHS England, but also includes other deaths of patients who were confirmed cases, whether they died in hospital or elsewhere. During the two weeks leading up to the change, the previous series of hospital deaths was 15% lower than the new series of Covid-19 deaths in all settings. The new data will still generally show a smaller number of deaths than deaths reported by the Office for National Statistics (ONS), which are based on the causes of death recorded on death certificates. These can include cases where the doctor thought it likely that the person had COVID-19, even when there was no positive test result.[2] The ONS data is provided with a considerable lag, because it takes at least 5 days for a death to be certified by a doctor, registered and the data processed. The most recent data from the UK Office of National Statistics from death registrations (Statistical Bulletin, Deaths registered weekly in England and Wales, provisional: week ending 1 May 2020, ONS 12 May) suggests that the cumulative number of Covid-19 deaths reported by PHE (by 1 May) understate the death registration number by about 20%.
With those qualifications, Figure 1 shows the log-change in deaths by days since the lockdown in each country. A similar picture emerges when looking at days since the 50th death occurred in each country. It is clear that there is increasing correspondence between daily log-change in the number of deaths in the three countries as the days since the lockdown increase, and the curves for Italy and Spain have flattened. We focus on Italy as the comparison country for the UK because it is 5 days further along in the development of the epidemic since the lockdown than Spain, and Spain’s daily proportionate change in the number of deaths is on a similar path as Italy’s. For forecasting purposes it makes no difference whether we comparing with Italy using days since the 50th death or since the lockdown. The ‘likely progress’ or ‘forecast’ assumes that the log-change change in the UK during the 14 days following the last observed data (on 17 May here) is the same as that in Italy on the corresponding day since Italy’s lockdown or its 50th death. This does not impose that the UK reaches the same level of Covid-19 mortality as Italy, only that it in the future it changes in the same way during a comparable stage of the epidemic. This procedure forecasts 38,000 UK deaths in all settings using the PHE measurement by 31 May compared with 34,636 deaths reported by PHE by 17 May. In light of the aforementioned under-count of all deaths from PHE reports, we can however expect a full total of around 49,000 registered Covid-19 deaths by this date.
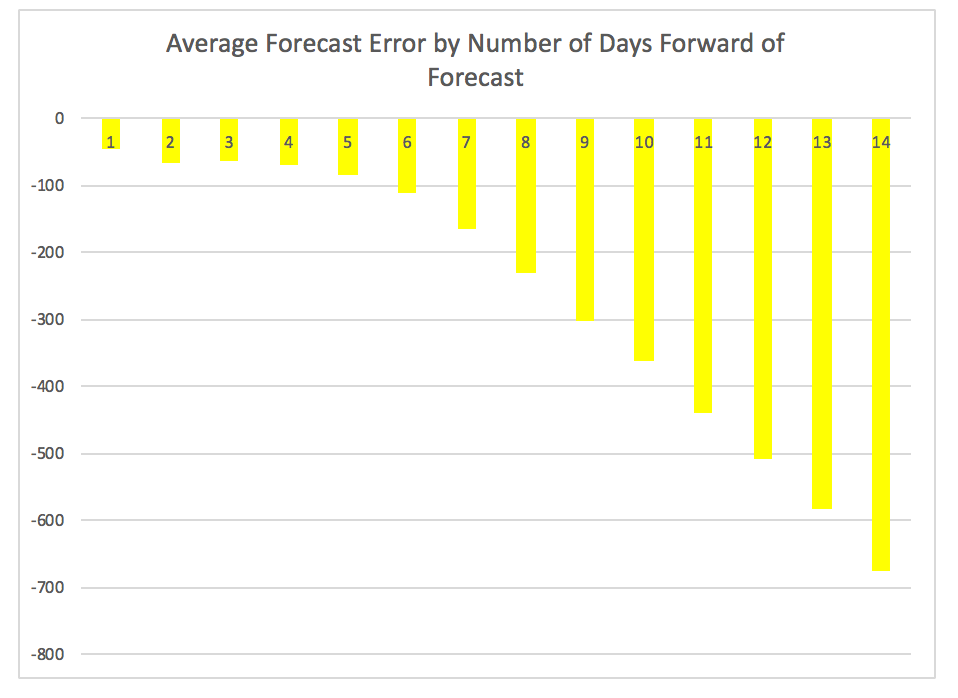
An analysis of forecast errors for deaths from using this approach strongly suggests that the forecast of 38,000 for 31 May is probably an understatement of actual deaths by then. Averaging over the forecasts from the one based on 7 April to the one based on 15 May, Figure 2 shows the average errors by length of forecast. The averages are all negative and increase with the forecast horizon, although they are not very large considering the forecast horizon, being under 700 deaths for forecasts up to 14 days ahead. The most recent forecast converted into a popular ‘headline’ figure, daily reported deaths, suggests that there will be about 230 deaths per day around 31 May, the lowest the lowest 7-day average since 30 March.
[1] e.g. Estimating the number of infections and the impact of nonpharmaceutical interventions on COVID-19 in 11 European countries by the Imperial College COVID-19 Response Team, 30 March 2020 [2] The deaths reported by ONS will include deaths that are not included in the PHE definition, because they had no positive test result confirmed by a PHE or NHS laboratory. They may also exclude cases that are included in the PHE definition because although the patient had a positive test for COVID-19 this was not mentioned on the death certificate. However, in general, the numbers of deaths reported by ONS will be larger than those included in the PHE definition.
Figure 1. Daily proportionate change in number of Covid-19 deaths by days since the country’s ‘lockdown’ (9 March in Italy, 14 March in Spain and 23 March in the UK).

Figure 2. Average forecast error for cumulative deaths by day of forecast horizon
Excess Deaths in England and Wales
The impact of the Covid-19 virus on mortality could be more, or less, than the number of deaths in which Covid-19 was mentioned on the death certificate. There are different ways to calculate ‘excess deaths’ corresponding to a disease. First, the time frame of the calculation matters because deaths may just be brought forward, say during a year, and so the excess deaths for the year is probably a more meaningful figure than the same calculation over a shorter time frame. Second, there must be a ‘counterfactual’; i.e. what would deaths have been had the disease been absent? Using death registration data up to 1 May England and Wales, Figure 3 shows excess mortality for each of the first 18 weeks of 2020 using average deaths during the previous 5 years in the corresponding week as the counterfactual. It indicates negative excess deaths from mid-January to mid-March. After 13 March, excess deaths rose sharply, as did Covid-19 deaths, peaking in the week ending 17 April, during which registered deaths were 113% above average. It is possible that some of the excess deaths since 13 March are ‘deaths postponed’ from earlier in the year. For instance, during the pre-epidemic period up to 13 March, 65% of the shortfall in deaths relative to the 5-year average are accounted for by 3,200 fewer deaths from respiratory causes. To take better account of such intertemporal substitution we measure excess deaths as deaths during the first 18 weeks of 2020 above the 5-year average for these weeks. On this accounting, excess deaths in England and Wales were 41,670, or 20% above average. Covid-19 deaths during the same period were 33,370. Thus, in addition to the Covid-19 deaths during the period there were another 8,300 deaths above average. If we had only looked at the period since 13 March, as many newspapers report, we would obtain 46,570 excess deaths, or 64% above average.
Figure 3: Weekly Excess deaths and Covid-19 deaths during 2020, England and Wales

Figure 4 illustrates a high concentration of excess deaths among the over-75s, but their proportion of excess deaths is not much larger than their average proportion of deaths in the past (74% cf. 70%). The difference between the height of the bars measures excess non-Covid deaths, which are more concentrated among the over-75s than excess deaths (81%).
Figure 4: Excess Deaths and Covid-19 Deaths in the first 18 weeks of 2020 by Age

Figure 5: Excess Deaths and Covid-19 Deaths per 100,000 population in the first 18 weeks of 2020 by Region

Figure 5 shows excess deaths and Covid-19 deaths per 100,000 population by standard regions. London, the West Midlands and the North West have experienced proportionately much more excess mortality than elsewhere. These three regions account for 48% of all excess deaths, but they constitute only 37% of the population of England and Wales. The West Midlands and North West have a particularly large number of excess deaths per 100,000 population not accounted for by Covid-19 deaths (the difference between the bars in Figure 5).
Figure 6 illustrates the higher incidence of excess deaths among men (60% of excess deaths) and a larger proportion of excess deaths at ages 45-64 among men than women (28% cf. 21%).
Figure 6: Excess Deaths in the first 18 weeks of 2020 by Age and Gender

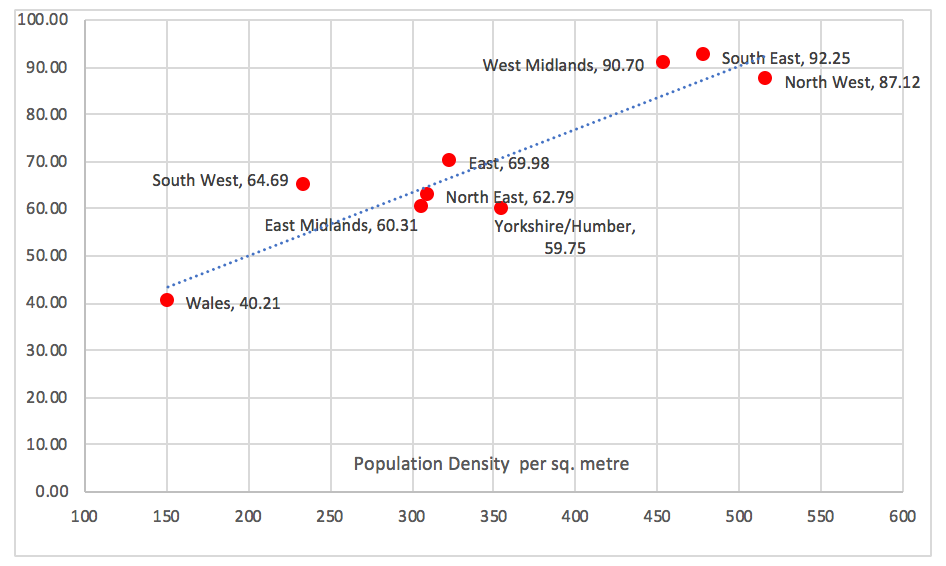
Figure 7 shows excess deaths per 100,000 population by standard regions outside London and its strikingly strong relationship with the region’s population density. The reason for the strong positive relationship appears to be the higher chance of Covid-19 infection in denser populations. For instance, it contrasts with a significant negative correlation between population density and overall regional mortality in 2018. The South East, West Midlands and the North West have the highest excess mortality rates and densities, and Wales the lowest.
Figure 7: Region’s Excess Deaths per 100,000 population in the first 18 weeks of 2020 and Region’s Population Density (correlation coefficient=0.92)
Confirmed cases
As with Covid-19 mortality, the outlook for confirmed cases relies on the development of cumulative confirmed cases in countries further along in the epidemic (Italy and Spain). Cumulative confirmed cases is a leading indicator of the progress of infection, even though we know it understates the true number of infections by an order of magnitude. For example, as of 28 March 2020, the Imperial College Team (Table 1) estimated that around 3% of the UK population was infected, compared with the percentage of confirmed cases of 0.03% on that date. (Estimating the number of infections and the impact of nonpharmaceutical interventions on COVID-19 in 11 European countries by the Imperial College COVID-19 Response Team, 30 March 2020).
Two approaches were considered, differing in their base point for measuring ‘epidemic time’ (t=0): (a) when the country reached 200 cases (24 February in Italy, 4 March in Spain and 7 March in the UK), or (b) when the country imposed its ‘lockdown’ (9 March in Italy, 14 March in Spain and 23 March in the UK). As Figure 9 illustrates, Italy and Spain appear to be converging to a similar path in terms of daily log change in cumulative cases using either approach, but they also indicate that, while flattening, the UK’s proportionate daily increase in confirmed cases remains above Italy’s and Spain’s at comparable advanced stages of the epidemic. This might be because of the rapid increasing in UK testing during recent weeks, which may be uncovering increasingly more confirmed cases, but we cannot be sure.
We focus on Italy as the comparison country for the UK because it is 7 days further along in the development of the epidemic than Spain. The ‘likely progress’ or ‘forecast’ assumes that the log change in the UK during the 14 days following the last observed cases data for the UK is the same as that in Italy on the corresponding day since Italy reached (a) 200 cases or (b) the lockdown. These forecasts using the 17 May base data show the UK reaching (a) 256,000 or (b) 259,000 confirmed cases by 29 May. The latter approach, which forecasts further into the future, suggests that there will be 260,000 cases by 31 May. In terms of a 3-day moving average of daily new confirmed cases, this amounts to 900 new cases per day around 31 May.
This approach does not readily accommodate the production of a confidence interval for the forecast. We can however ask, for example, how well does each 12-day forecast predict the actual outcomes. Figure 10 answers this question for approach (a). It shows the average forecast error for each day of the 12-day forecast horizon averaging over forecasts produced from 27 March through the forecast on 27 April, which is before the big increase in virus testing. Beyond day 2 of the forecast, the forecast error is always negative as the averages in Figure 10 suggest, and the understatement increases with the forecast horizon, averaging 14,900 for the 12-day forecast.
There is a clear tendency for the forecasting procedure using approach (a) to understate the number of cases, making it a lower bound, or ‘best case’ scenario. As the forecast from approach (b) is not much larger than the one from approach (a) it is also likely to be conservative (i.e. too low). The amount that it undershoots future confirmed case is undoubtedly increasing because the UK’s and Italy’s paths for cases have diverged (as Figure 11 illustrates), making the forecast less useful for anything but a lower bound.
Figure 8. Daily log change in confirmed cases measured from days since the country’s ‘lockdown’ (9 March in Italy, 14 March in Spain and 23 March in in the UK).

Figure 9. Average forecast error by day of forecast horizon using approach (a)

Figure 10 shows that the UK’s proportionate rate of increase in confirmed cases remains well above other large European countries at about 1.4% per day (about 3,400 cases) compared to 0.6% in Spain and under 0.5% in the other three countries. All these countries had begun easing their lockdown by at least 13 May, making it interesting to compare developments in new cases during the coming weeks.
Figure 10: Daily proportionate increase in confirmed cases since beginning of May, 3-day moving average

